Dahatre wrote:Models are as good as the underlying assumptions. Not being an epidemiologist, I am not even sure some things can be modeled. Learned in my zoom journal club jana that unlike earlier reports, it now seems like this virus has mutated
and some strains of the virus are deadlier than others--If true, how do you model mutations?
P/S waiting (hoping/praying) for KEMRI to tell us that we have the less virulent strain...
Yes, Models are as good as the underlying assumption and having one global model to try and determine the outcome of how 7 billion people and the various systems they put in place and their relations is not a simple task. The above model is very likely wrong on the dates but its worth looking into and feeding data. It surely beats pulling figures from the top of the head and saying it has infected 1,000,000 people.
On mutations - yes - you cannot model out the outcome of Mutations.
Since Viruses need to execute 3 steps really well in order to go 'viral'
1) infect - a virus has to infect a host
2) replicate - a virus has to use that host's cell replication mechanism to replicate
3) escape the host - the kid viruses have to get out of that host into another host to start step 1 of the new host.
But since they are billions of these viruses around and each time they execute the replication stage there is a chance that they may mutate and each mitation may have one of 3 outcomes on the fate of the kid virus.
1) it may be disavantageous - the virus may lose something it's parent had and cannot infect the cells of the animal its currently on and the body kills it. or may gain some capability to kill off the cells it infect early before it reproduces or may lose the coding that enables it to be spread through the channels the parent used to infect the current host.
2) it may be neutral - a change that does not affect the 3 stages. the host continues behaving the same way and passes on the kid virus to the next host etc. the parent and kid happen to be slightly different
3) it may be advantageos to the virus - it may infect different type of cells and get multiple channels to leave the body. it may change in a way that the immunorespose of the host is no longer able to kill it.
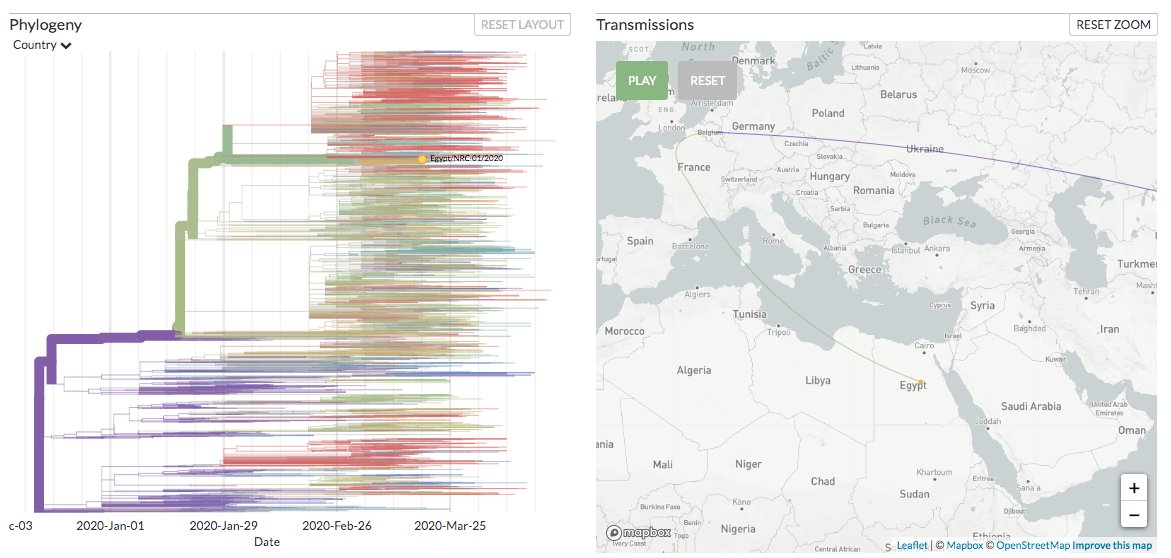
While to my knowledge there are 2 strains -(S and L) of Covid... there are hundreds possibly thousands of mutations of the virus. these minute changes in their genome enable people like the guys running this website
https://nextstrain.org/ncov
track where the virus in a certain country came from. here is an example of how a virus sequence submitted from Egypt relates to other viruses
kaka2za wrote:
Fact: Fatalities in Africa REMAIN far less than was expected.
Reason: matter of conjecture
Don't legeza kamba!
All Mushrooms are edible! Some Mushroom are only edible ONCE!